– “ Do you place Immediates in the aesthetics zone?”
– “Do they work? Is it a treatment option to pursue or to avoid?”
For the first question my response would be rather short. For the second however I will need more of your time and attention!
… so let me explain my thoughts on this!
In other words, when it comes to aesthetic zone implants the question is not only “to go immediate or not” but also what kind of immediate procedure one would follow.
When conditions allow, an immediate implant can be placed flapless in the Aesthetic zone and consequently be restored immediately with a temporary crown. This technique and its outcomes are well documented among other through a prospective study we initiated some years ago in Australia [1], which has now been expanded with published data after a mean of four years of observation [2] . Of course, the flapless immediate implant which is to receive an immediate temporary crown is a highly complex procedure and certain strict criteria with regards to the local anatomy and the patient selection need to be applied. These criteria are very well described in a recent paper by Buser et al. [3] (Table 1).
Selection criteria for Imemdiate Implant:
– Intact facial bone wall with thick phenotype (>1mm)
– Thick soft tissue biotype
– No acute infection in the socket
– Sufficient bone volume apically to stabilise the implant in the correct position
– Flapless placement if possible
Table 1. Adjusted by Buser et al [3]
The interdental papilla is the most voluptuous part of the periodontal soft tissues and requires a rich vascularisation through anastomoses of 4 different sources of blood supply: the Periodontal ligament of the two neighboring teeth and the buccal and palatal bloodstream. Any cut and detachment of the soft tissues will result is disturbance of the blood flow and irreversible compromise of the architecture, as anastomoses between the buccal and the lingual flap are significantly reduced post extraction or surgery [4] . A flapless placement, when possible, allows for the minimal disturbance of the soft tissues, as buccal and palatal soft tissues are not cut or detached, while the interdental papilla maintains vascularisation from the existing anastomoses and the neighboring tooth’s alveolar bone and periodontal ligament. This way the interdental tissues maintain three out of the original four sources of blood supply after the extraction, having only lost the periodontal ligament of the extracted tooth.
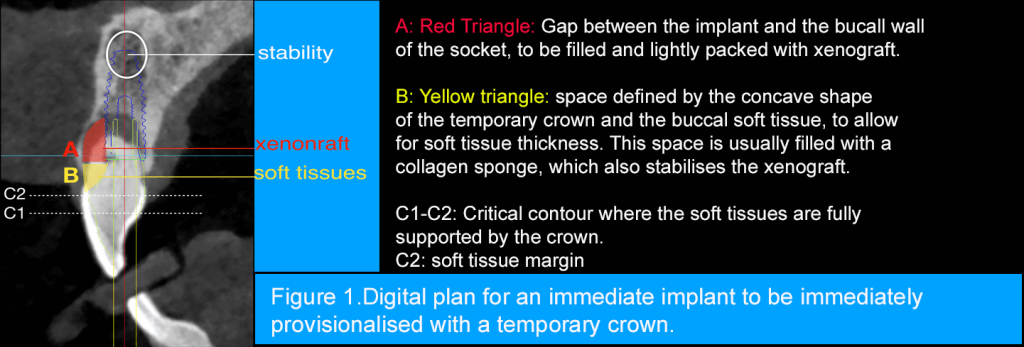
When supplemented with an immediate crown, which supports the soft tissue replicating the shape of the extracted tooth, one can expect the best possible chance to maintain the soft tissue architecture. Such an immediate crown, is usually designed concave at its base in order to allow the space for the ingrowth of thick soft tissue. It will gradually thicken in order to replicate the contour of the tooth as it comes in contact with the first 2-3 critical millimetres of the soft tissues facing the socket and the papillae (Figure 1). If an immediate temporary crown is for any reason not possible or desirable, the same results can be achieved with a custom made healing abutment, which will replicate the contour of the tooth and support the soft tissues, while not exceeding the marginal tissue height.
Does this technique guarantee tissue stability? Of course not, but 5-year prospective results published in 2017 by the group of Professor Ivanovski in Australia [2] can help quantify the risks we are facing and support decisions. After 4-5 years the percentage of implants which lost more than 1.5 mm of soft tissue was around 5% or less, while the great majority demonstrated very good stability of both papillae and mid-buccal tissues. Similarly, the percentage of implants that lost between 1.5-2 mm of bone height for the same period of observation was around 6 %, while many implants showed bone gains. At the same outcomes, Pink Eshetic scores improved in the observation perios and were on average very high, with a score of 11.
Also observe that this technique does not involve an actual GBR approach (membrane), as we do not raise a flap or mobilise tissues. A minor augmentation of the gap in the extraction socket is only performed and the area is stabilised with the temporary crown and often some collagen sponge (Figure 1).
Let’s look now at the other option, placing an immediate with a flap in the Aesthetic zone, which is also by now well studied [5-7]. One might wonder, “Are things so different if we do an immediate implant with a flap?”
-Yes, I believe there are two major differences when we raise a flap around an extraction socket.
First, like we mentioned previously, cutting and detaching the soft tissues will inevitably and irreversibly change their integrity and architecture.
Even under the most delicate and precise surgical manipulations, healing – which is essentially a repair- will involve a certain extent of scar tissue. This is shown to reduce anastomoses and compromise the microvascularization of the healed issues. Inevitably, the risk of early unfavorable changes in the tissue architecture and esthetics is significant when an immediate implant is placed with a flap.
Second -and maybe even more important- around the fresh extraction socket there is never enough soft tissue to achieve a complete closure of the flap, especially when GBR is conducted.
Significant manipulation of the flap is required in order to achieve primary closure, as the diameter of the socket in the aesthetic zone is much larger than that of the implant placed immediately. Such manipulation usually involves some coronal advancement or release incisions and will inevitably further compromise the soft tissue topography, possibly also affecting the zone of keratinized mucosa and tissue thickness.
Consequently, based on these two parameters, it is not surprising that immediate implants when placed under a flap and combined with GBR will result in higher risk for tissue changes and poor aesthetic outcomes. Tonetti et al in a carefully designed study published recently [7] found 42 % of the implants placed with this technique presented below acceptable pink aesthetics scores, which was set at a score of 6 or less. The authors concluded that delayed placement was a much safer option, with only 19% of the implants having below acceptable pink aesthetics scores.
So, dear colleagues, since you have bothered to read that far, maybe it’s time for me to sum up and present you with my response to the questions we started this article with:
–Yes, I do place immediate implants in the aesthetic zone, but only if all the conditions are there to allow me to place them flapless and provide an immediate temporary crown, or at least a custom-made healing abutment. I consider this is a minimally-invasive and predictable technique, but unfortunately the strict selection criteria also mean that only 5 to 10 % of the aesthetic cases in my practice will end up receiving such an implant.
For the remaining cases I will extract the tooth, leave the socket to heal undisturbed and place the implant with simultaneous GBR after 6 to 8 weeks. In my practice the early placement with GBR remains still the “Working Horse” of the Aesthetic zone, although flapless immediate implants are not uncommon. Immediate implants under a flap is a choice I would rarely justify today in the aesthetic zone, based on both experience and now also significant published evidence.
As the digital -surgical and prosthetic- workflow advances, maybe soon immediate implants and temporaries will have an increasing role and more indications in implant practice.
If you’re interested to discuss this topic further, please feel free to mail me or even better come and join our upcoming 2-day course 4-5 May 2019 , for which you can find out more here!
Thank you for your time
Nikos
References
- Khzam N, Mattheos N, Roberts D, Bruce WL, Ivanovski S.Immediate placement and restoration of dental implants in the esthetic region: clinical case series. J Esthet Restor Dent. 2014 Sep-Oct;26(5):332-44.
- Arora H, Khzam N, Roberts D, Bruce WL, Ivanovski S. Immediate implant placement and restoration in the anterior maxilla: Tissue dimensional changes after 2-5 year follow up.Clin Implant Dent Relat Res. 2017 Aug;19(4):694-702.
- Buser D, Chappuis V, Belser UC, Chen S. Implant placement post extraction in esthetic single tooth sites: when immediate, when early, when late? Periodontol 2000. 2017 Feb;73(1):84-102
- Cranin AN1, Sirakian A, Russell D, Klein The role of incision design and location in the healing processes of alveolar ridges and implant host sites.Int J Oral Maxillofac Implants. 1998 Jul-Aug;13(4):483-91.
- M.Sanz M1, Cecchinato D, Ferrus J, Pjetursson EB, Lang NP, Lindhe J. A prospective, randomized-controlled clinical trial to evaluate bone preservation using implants with different geometry placed into extraction sockets in the maxilla. Clin Oral Implants Res. 2010 Jan;21(1):13-21.
- Huynh-Ba G, Pjetursson BE, Sanz M, Cecchinato D, Ferrus J, Lindhe J, Lang NP. Analysis of the socket bone wall dimensions in the upper maxilla in relation to immediate implant placement. Clin Oral Implants Res. 2010 Jan;21(1):37-42.
- Tonetti MS, Cortellini P, Graziani F, Cairo F, Lang NP, Abundo R, Conforti GP, Marquardt S, Rasperini G, Silvestri M, Wallkamm B, Wetzel A. Immediate versus delayed implant placement after anterior single tooth extraction: the timing randomized controlled clinical trial. J Clin Periodontol. 2017 Feb;44(2):215-224.