How wandering in the forest can pave the way for successful implant surgeries
by Nikos Mattheos, DDS, MASc, PhD and
James Chow, BDS, MDS, FRCDSE(OMFS), FRCDSC(OMFS)
Back in my days in the Boy Scouts, orienteering was one of the most exciting activities. We would pick a high spot and sit under a shadow, then unfold a paper map on the ground next to the compass. Looking at the map for a few minutes, looking around and plotting some lines was enough for us to walk for hours until the next checkpoint, or our final destination.
Several decades later and finding my way in the forest is a childhood memory. But could this experience have laid a foundation to help me become a better implant surgeon? The answer is “yes” and the codename is “SRA” or better “Spatial Representation Ability”.
Have you ever thought why some people are fast to orientate with a map, while others tend to be always lost? Or, why some prefer to look at the navigation carefully once before driving, while others need to have it constantly in front of their eyes? And what does this all have to do with implant surgery? I think I have some answers for you today!
Thinking back of these days with some of my best friends running around the forest, I recall a strong feeling of challenge and achievement. We thought we were competing in a treasure hunt, but looking back however with what I know now, I can see the traits of what we were really learning and what the true reward was. I remember how we were “growing” in the task. At start we needed frequent stops and checks, there was doubt and ambivalence when confronted with unexpected furcations of the road, disagreements. But we grew fast. Stops became less frequent, certainty increased, the team could walk for hours without wasting time to take out the map. Some people emerged who were really good at it, they were fast with reading the map and they were right most of the time on the path. At that time we thought they had a better “sense of direction”. Today however, I have a better description: these kids had just managed to develop higher a very common skill called Spatial Representation Ability. Later on, I noticed that teams which had a strong pathfinder, tended to stagnate, as the other members often relied on the authority of the expert pathfinder and did not share the challenge. Thus, as a leader one had to reshuffle the teams often. In the end, the whole troop would grow and everyone was able to walk in and out of the forest with a map and a compass.
(PS: 20 years later and the same observation comes back from a different source, as a study from UCL pointed out how reliance on real time GPS makes drivers less able to find their way in a city…We have to find ways to use tools and expertise to make us wiser, not dummer!)
So what is this Spatial Representation Ability?
Spatial representation ability is a cognitive skill, which helps us reconstruct a 3-dimensional space out of a “representation” which can be a 2D photo, a map or any other encoded information. It’s not the typical “imagination”. It’s a cognitive skill, which implies that you only need two things to master it: a brain and training! In particular, neuroscientists have pinned this skill to the neurons of the hippocampus, medial temporal lobes and posterior parietal cortex, areas of the brain often associated with planning movements and making decisions about images in the field of view. These areas of the brain demonstrate high plasticity: synaptic connections are constantly restructured in response to stimulation. You can practice in million ways, but the recipient “muscle” you strengthen is the same. Nobody is born with a good “sense of direction”, only with a highly “plastic” brain. We all start building up our SRA from the moment we are born in countless different ways. Like an expert musician reads notes in paper and hears music in his mind, SRA is the skill to mentally recreate a building from a drawing or a forest from a map and place yourself in this space, helping you to navigate it with success. But it’s not enough to have the drawings only, you need to match the drawings and the forest – again and again – in order to grow the skillset. In dental admission in US, spatial representation ability tests have been utilised successfully for over than 40 years, showing good correlation with early manual skills.
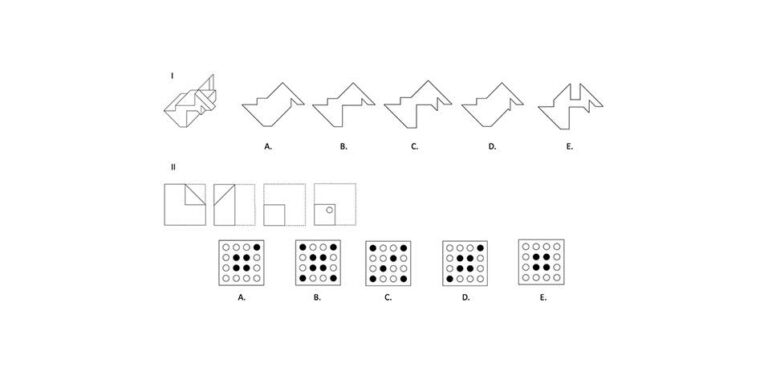
Perceptual Ability Test (PAT), has been utilised for more than 40 years on Dental Admission Test (DAT) in USA. It is a pencil and paper test aiming to measure spatial ability, although not in anyway specific to or related to dentistry. It has been proposed to be a valid predictor for predicting success in the manual skills of dental curricula
Now what does this all have to do with Implant Surgery?
A whole lot, as long as surgery is a process directly depending on our ability to understand anatomy. Evidence shows that the ability to precisely synthesize and cognitively project local anatomic structures in 3-dimensional (3D) space, detailing the shape of each anatomical element, the relative locations and how these structure are connected in that space is a skill that can be learned and a key competence in the training of implant surgeons.
Surgical anatomy is a dark box, until the moment we raise a flap and we see what lies under the skin. Rather than cutting our way to find out however, we use “representations” like photos and radiographs to mentally reconstruct the anatomic space and plot the optimal path in this biological forest. Unfortunately, much of our early learning of anatomy relies mainly in memorizing endless names and relations; a task for which I can be eternally grateful that I had Greek as a mother tongue. If you were lucky enough to do full cadaver dissections during your anatomy training, it is then that you get a feel for the first time how the real forest looks like and you get to know that veins are not really blue and nerves not yellow. But finally, when you cut with the blade for the first time, it is then that you can place everything in context and feel the value of a single millimetre. From this point on, your SRA as a surgeon is only growing. With training and growing experience you will soon read a radiograph like an expert musician reads his notes: you will not hear the music, but you will “see” the actual bone for 3D the shape it is.
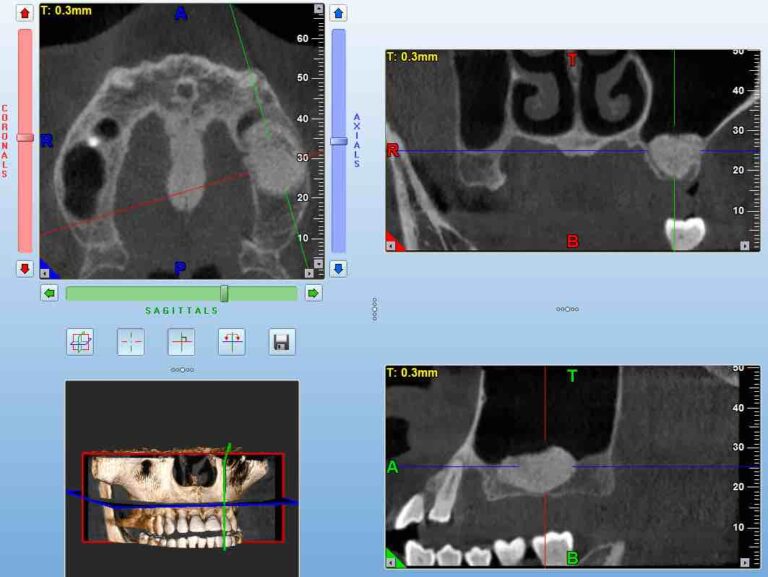
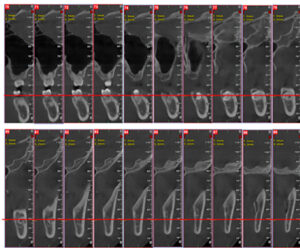
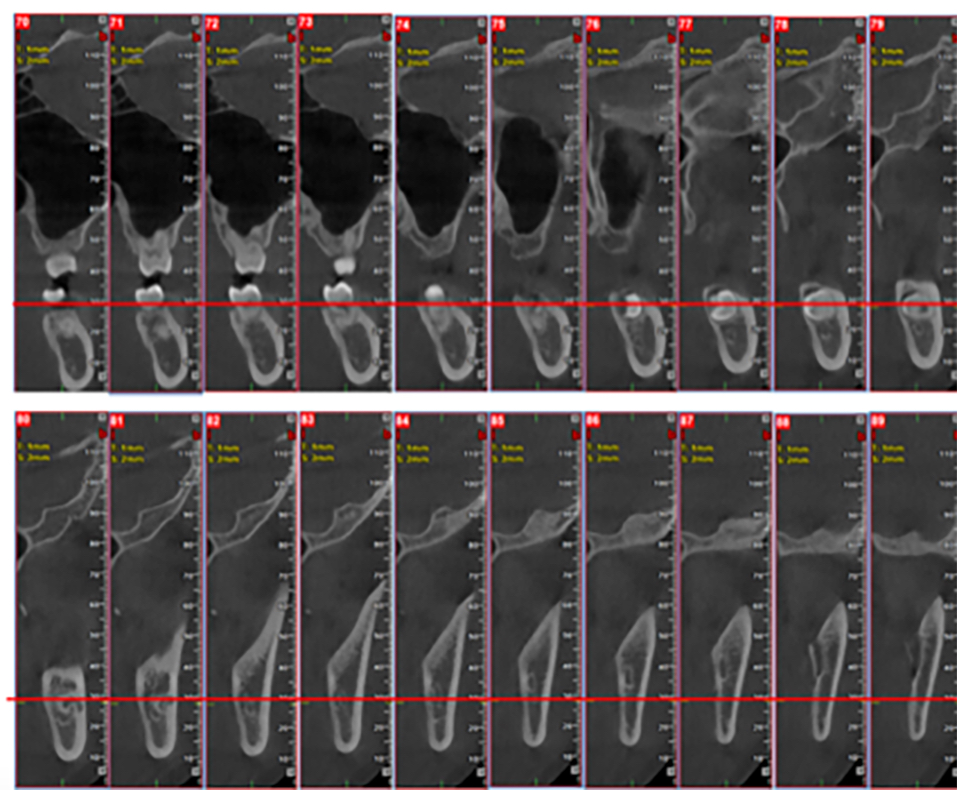
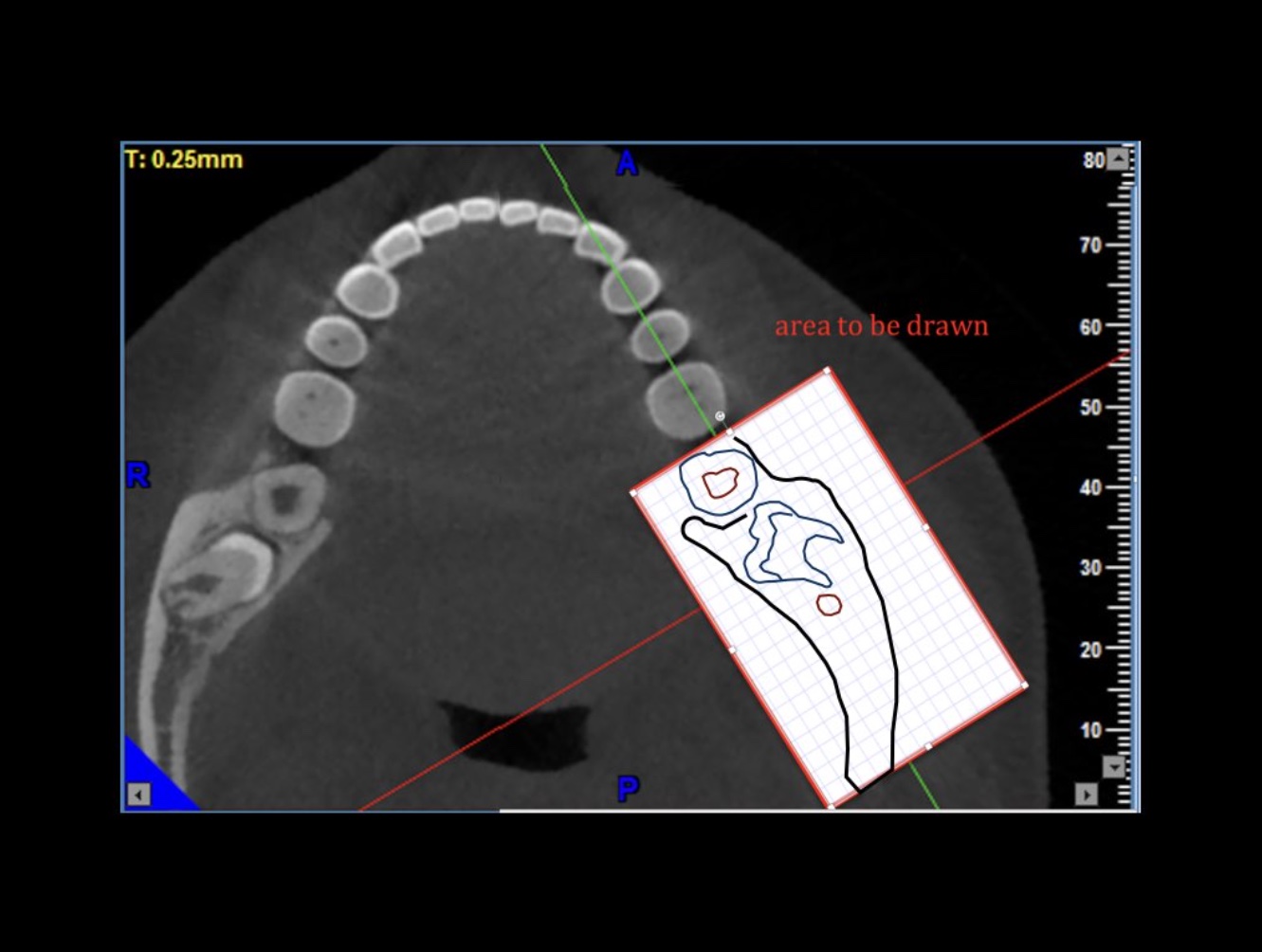
A Cone Beam CT is compiling 3D data, but it still allows us to access it only through 2d representations (slices) in a flat 2D screen. The surgeon has to read these combined 2D images and reconstruct a mental 3D structure of the surgical anatomy, certainly not an easy task to do with precision.
Raising your spatial representation ability is raising your surgical performance
There is only one way and this is training. To maximise the effects of training however and to train others fast and efficiently, you need to leave nothing to chance. The principle strategy is to study carefully the available representations and try and mentally visualize it in advance in 3D. In particular today with the 3D radiographic imaging and tomographies, combined with optical scanning we have some unique representations.
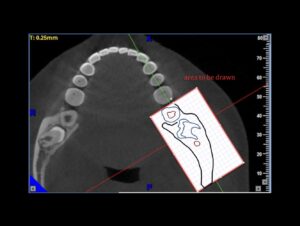
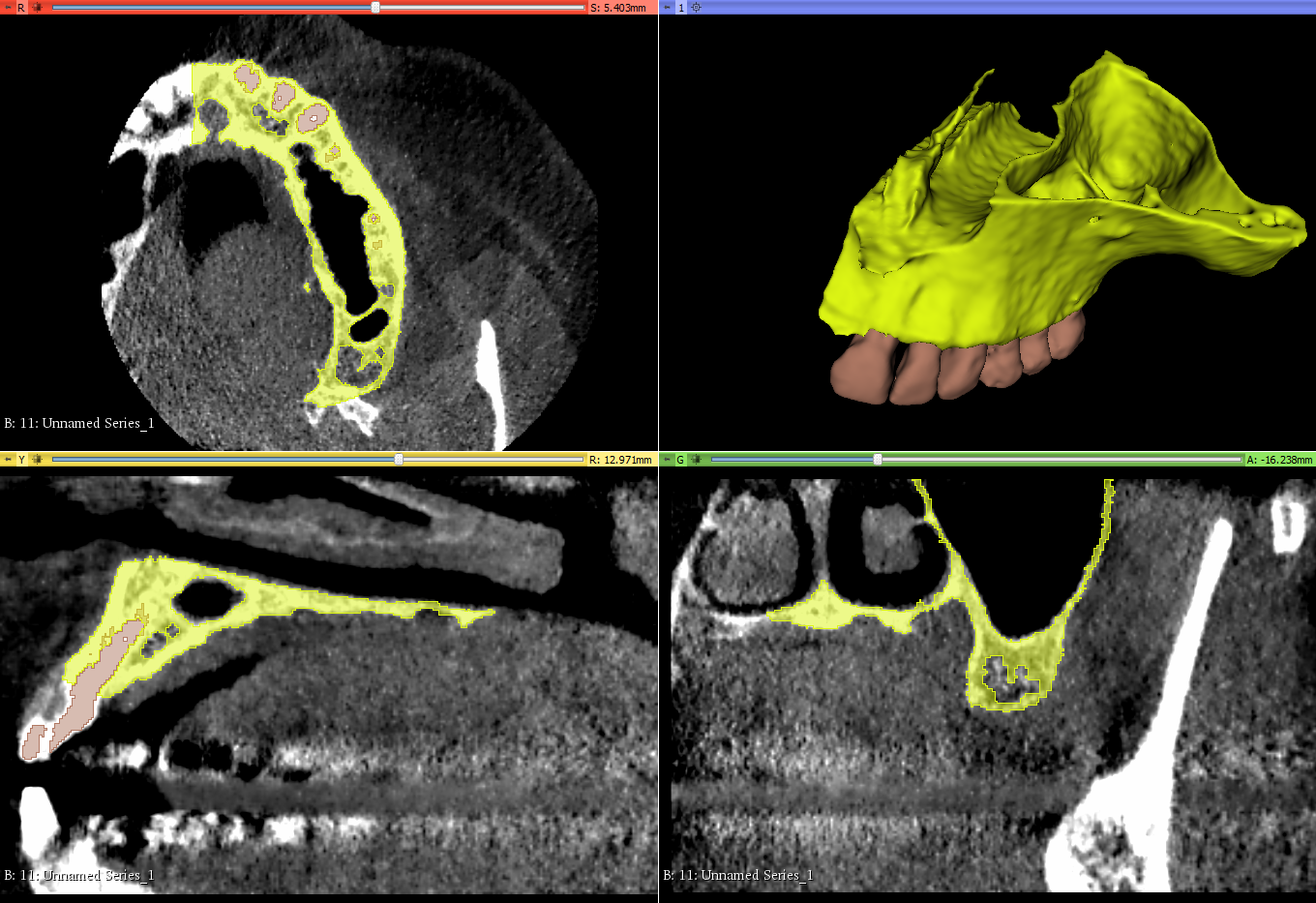
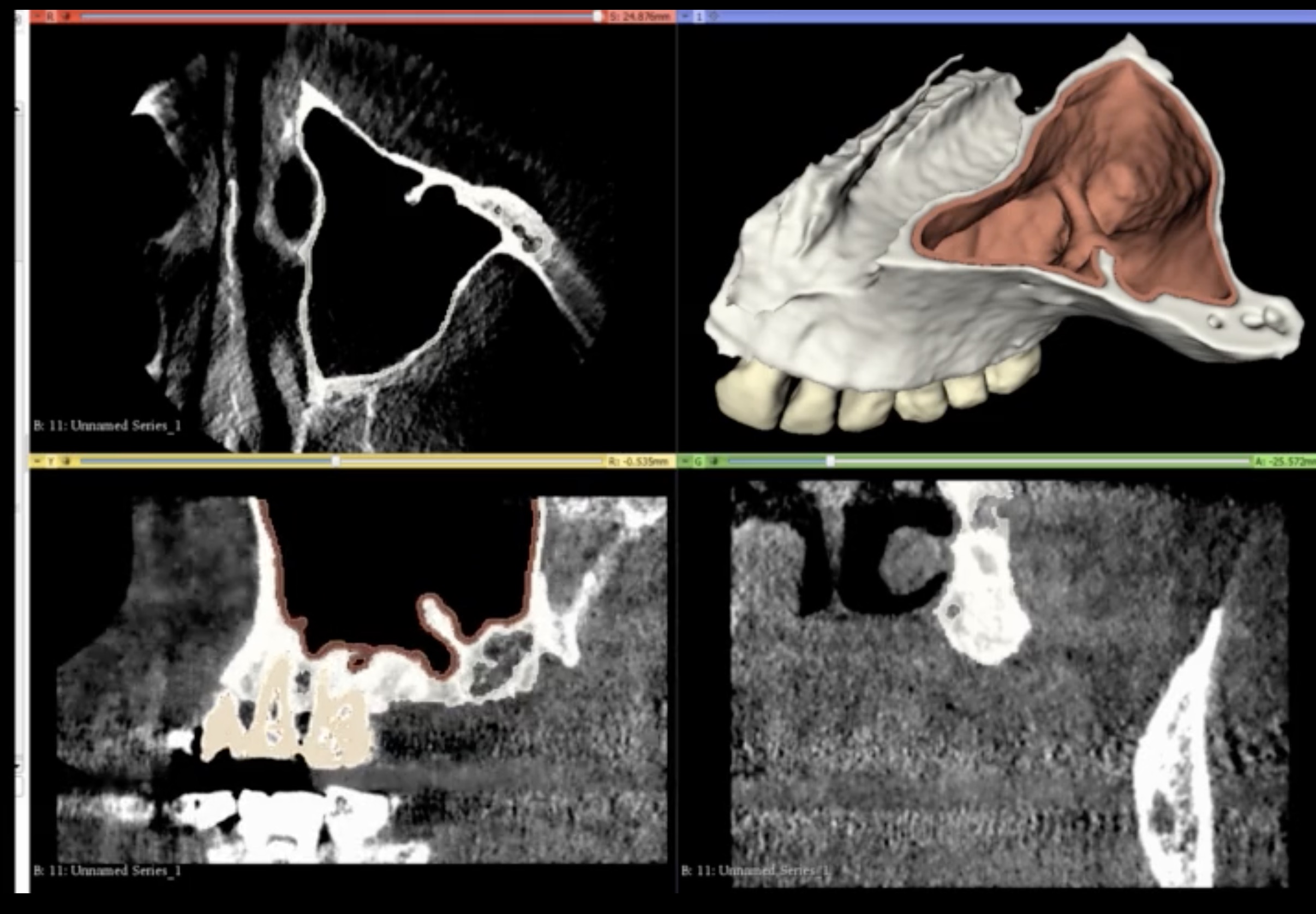
Note here that although the data we aquire from a CBCT are 3-dimensional, in reality the representation is still 2D: we only see it in a flat screen. To recreate a truly 3D representation you will need to 3D print the data from the CBCT. This is actually a very powerfull teaching medium, which we have often utilised in complex surgeries. 3D printing the anatomy prior to surgery allows you to test different techniques and access points with safety, before you choose the best way to go in (or sometimes to not go in at all).
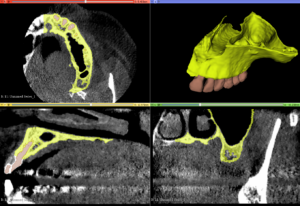
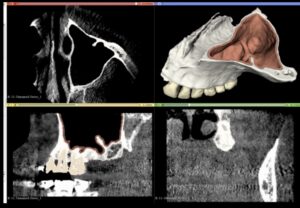
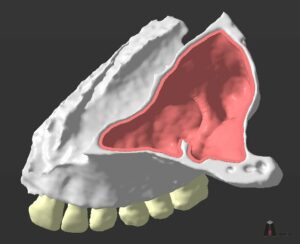



A Challenging surgical case with a complex of vertical and horizontal septa in the posterior sinus. Segmentation of the 3D radiographical and optical data and 3D printing in multiple layers from AMMA Ltd Hong Kong, has allowed for an accurate representation of the anatomy where multiple surgical access approaches were tested.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Find out how good you are!
An important question for everyone. Do not mix SRA with other surgical skills such as cutting and suturing, SRA is an underlying skill. It will “naturally” grow with every surgery, but if you want to excel it you have to target it with specific training, just like anything else. And if you want to test your level, you also need some specific test. Many tests are available to test SRA, most of them are very generic though. Some time ago with Dr. James Chow and Dr. Coral Yao we developed a test specific to understanding surgical anatomy with the use of CBCT. The challenge here is to reconstruct a 3Dimensional anatomic space from 3 2D representations, as we routinely have to do while “reading” a CBCT. The test was called DASRA and was scientifically validated. It will give you an idea of the level of an important skill for implant surgery and it’s available online for free. Take the DASRA challenge and remember to leave us your thoughts and comments.
In conclusion, having been a Scout will help you
become a better implant surgeon, landscape architect,
civil engineer and any other profession you can think of.

Hear the latest news first, subscribe now to my newsletter!
References
1. Yao CJ, Chow J, Choi WWS, Mattheos N. Measuring the impact of simulation practice on the spatial representation ability of dentists by means of Impacted Mandibular Third Molar (IMTM) Surgery on 3D printed models. Eur J Dent Educ. 2019;23:332–343
2. Schultz, Robins M, Markowitz K, DeCastro J, Jiang S. Comparison of Dental Students’ PAT scores with their performance in preclinical technique courses: identifying the need for early interventions. J Dent Educ. 2018;82:406‐410.
3. Hegarty M, Keehner M, Khooshabeh P, Montello DR. How spatial abilities enhance, and are enhanced by, dental education. Learn Individ Differ. 2009;19:61‐70.
4. Berney S, Bétrancourt M, Molinari G, Hoyek N. How spatial abilities and dynamic visualizations interplay when learning functional anat‐ omy with 3D anatomical models. Anat Sci Edu. 2015;8:452‐462.
5.Javadi, A.-H. et al. Hippocampal and prefrontal processing of network topology to simulate the future. Nat. Commun. 8, 14652 doi: 10.1038/ncomms14652 (2017).